
Cortical bridging a union predictor: A prospective study after intramedullary nailing of the femoral shaft fractures
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Published: 28 October 2022
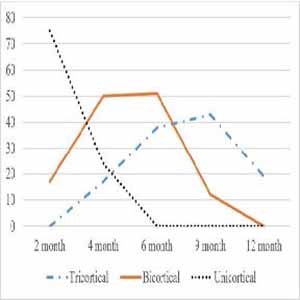
Early prediction of the union helps for timely intervention, reduction of hospitalization, treatment costs, and disability in cases of nonunion. With this in mind, we tried to find how long any cortical bridging predicts the union in femoral shaft fractures. A prospective study of 113 femoral shaft fractures treated with reamed, locked intramedullary nailing was performed. Radiographs were taken during months 2 to 4, 6, 9, and one-year follow-up. The cortical bridging (presence and number) was assessed by anterior-posterior and lateral views. The ROC curve provides the prediction of the union. The overall nonunion rate was 10.6% (12 of 113 fractures). Age and diabetes mellitus were statistically significant with nonunion (p value < 0.001). The final analysis demonstrated that any cortical bridging at four months postoperatively was the most accurate and earlier indicator (105 of 113, 92.9% accuracy), while it was 84.9% at six months in bicortical and 80.5% accuracy at nine months in tricortical bridging. Low-cost and simple radiographic imaging presents cortical bridging in any form 4 months after surgery that precisely predicts a union in femoral shaft fractures.
Downloads
Asplund CA, Mezzanotte TJ. Midshaft femur fractures in adults. UpToDate, Medilib, 2021. https://www.medilib.ir/uptodate/show/228
Rahman AF. The burden of road traffic injuries in South Asia: a commentary. J Coll Physicians Surg Pak. 2004;14(12):707-8.
Khan IA, Ahmad S, Shah MA, Ahmed S, Shafiq M, Shafaq SA. Static versus dynamic interlocking intramedullary nailing in fractures shaft of femur. Gomal Journal of Medical Sciences. 2015;13(2).
Omerovic D, Lazovic F, Hadzimehmedagic A. Static or dynamic intramedullary nailing of femur and tibia. Med Arch. 2015 Apr;69(2):110-3. Epub 2015 Apr 6. DOI: https://doi.org/10.5455/medarh.2015.69.110-113
Karadimas EJ, Papadimitriou G, Theodoratos G, Papanikolaou A, Maris J. The effectiveness of the antegrade reamed technique: the experience and complications from 415 traumatic femoral shaft fractures. Strategies Trauma Limb Reconstr. 2009 Dec;4(3):113-21. Epub 2009 Nov 21. DOI: https://doi.org/10.1007/s11751-009-0071-2
Basumallick MN, Bandopadhyay A. Effect of dynamization in open interlocking nailing of femoral fractures. A prospective randomized comparative study of 50 cases with a 2-year follow-up. Acta Orthop Belg. 2002 Feb;68(1):42-8.
Shroeder JE, Mosheiff R, Khoury A, Liebergall M, Weil YA. The outcome of closed, intramedullary exchange nailing with reamed insertion in the treatment of femoral shaft nonunions. J Orthop Trauma. 2009 Oct;23(9):653-7. DOI: https://doi.org/10.1097/BOT.0b013e3181a2a337
Fisher W, Hamblen D. Problems and pitfalls of compression fixation of long bone fractures: a review of results and complications. Injury. 1979;10(2):99-107. DOI: https://doi.org/10.1016/S0020-1383(79)80069-8
DeCoster TA, Miller RA. Closed locked intramedullary nailing of femoral shaft fractures in the elderly. Iowa Orthop J. 2003;23:43-5.
Devnani AS. Open reamed femoral intramedullary nailing–revisited. Eastern J Med. 2003;8(1):7-11.
Meena R, Kundnani V, Hussain Z. Fracture of the shaft of the femur: Close vs open interlocking nailing. Indian J Orthop. 2006;40(4):243. DOI: https://doi.org/10.4103/0019-5413.34504
Bashir A, Mir B, Halwai M, Qayum A. First experience with locked intramedullary nailing of femur in Kashmir. Internet J Orthop Surg. 2008;8:1. DOI: https://doi.org/10.5580/9a9
Nicoll E. Fractures of the tibial shaft. J Bone Joint Surg Br. 1964 Aug;46:373-87. DOI: https://doi.org/10.1302/0301-620X.46B3.373
Müller ME, Perren S, Allgöwer M, Müller ME, Schneider R, Willenegger H. Manual of internal fixation: techniques recommended by the AO-ASIF group: Springer Science & Business Media; 1991. DOI: https://doi.org/10.1007/978-3-662-02695-3
Bishop JA, Palanca AA, Bellino MJ, Lowenberg DW. Assessment of compromised fracture healing. J Am Acad Orthop Surg. 2012 May;20(5):273-82. DOI: https://doi.org/10.5435/JAAOS-20-05-273
Canale ST, Beaty JH. Campbell's operative orthopaedics e-book: Elsevier Health Sciences; 2012.
Tay WH, de Steiger R, Richardson M, Gruen R, Balogh ZJ. Health outcomes of delayed union and nonunion of femoral and tibial shaft fractures. Injury. 2014 Oct;45(10):1653-8. Epub 2014 Jul 7. DOI: https://doi.org/10.1016/j.injury.2014.06.025
Hierholzer C, Glowalla C, Herrler M, von Rüden C, Hungerer S, Bühren V, Friederichs J. Reamed intramedullary exchange nailing: treatment of choice of aseptic femoral shaft nonunion. J Orthop Surg Res. 2014 Oct 10;9:88. DOI: https://doi.org/10.1186/s13018-014-0088-1
DiSilvio Jr F, Foyil S, Schiffman B, Bernstein M, Summers H, Lack WD. Long bone union accurately predicted by cortical bridging within 4 months. JBJS Open Access. 2018;3(4). DOI: https://doi.org/10.2106/JBJS.OA.18.00012
Giannoudis PV, MacDonald DA, Matthews SJ, Smith RM, Furlong AJ, De Boer P. Nonunion of the femoral diaphysis. The influence of reaming and non-steroidal anti-inflammatory drugs. J Bone Joint Surg Br. 2000 Jul;82(5):655-8. DOI: https://doi.org/10.1302/0301-620X.82B5.0820655
Malik MH, Harwood P, Diggle P, Khan SA. Factors affecting rates of infection and nonunion in intramedullary nailing. J Bone Joint Surg Br. 2004 May;86(4):556-60. DOI: https://doi.org/10.1302/0301-620X.86B4.14097
Strotman PK, Karunakar MA, Seymour R, Lack WD. Any Cortical Bridging Predicts Healing of Supracondylar Femur Fractures After Treatment With Locked Plating. J Orthop Trauma. 2017 Oct;31(10):538-544. DOI: https://doi.org/10.1097/BOT.0000000000000887
Ma YG, Hu GL, Hu W, Liang F. Surgical factors contributing to nonunion in femoral shaft fracture following intramedullary nailing. Chin J Traumatol. 2016 Apr 1;19(2):109-12. DOI: https://doi.org/10.1016/j.cjtee.2016.01.012
Zura R, Mehta S, Della Rocca GJ, Steen RG. Biological Risk Factors for Nonunion of Bone Fracture. JBJS Rev. 2016 Jan 5;4(1):e5. DOI: https://doi.org/10.2106/JBJS.RVW.O.00008
Pearson RG, Clement RGE, Edwards KL, Scammell BE. Do smokers have greater risk of delayed and non-union after fracture, osteotomy and arthrodesis? A systematic review with meta-analysis. BMJ Open. 2016;6(11):e010303. DOI: https://doi.org/10.1136/bmjopen-2015-010303
How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.