Sharon E. Orrange,1 Ahmet Baydur,2 Leslie A. Saxon,3 P. Michael McFadden4
1Departments of Internal Medicine, University of Southern California (USC) Keck School of Medicine; 2Pulmonary Critical Care, University of Southern California Keck School of Medicine; 3Cardiovascular Medicine, University of Southern California Keck School of Medicine; 4Cardiothoracic Surgery, University of Southern California (USC) Keck School of Medicine, USA
Correspondence: Sharon Orrange, University of Southern California (USC) Keck School of Medicine 1520 San Pablo 1st Floor, Los Angeles, CA 90033, USA. E-mail: orrange@usc.edu
Key words: pericardial cyst, cough, video assisted thorascopic surgery.
Conflict of interest: the authors report no conflicts of interest.
Received for publication: 6 February 2011.
Revision received: 4 March 2011.
Accepted for publication: 8 March 2011.
©Copyright S.E. Orrange et al., 2011
Licensee PAGEPress, Italy
Chest Disease Reports 2011; 1:e1
doi:10.4081/cdr.2011.e1
AbstractPericardial cysts are rare mediastinal cysts and an uncommon cause of cough. Patients are often asymptomatic but can present with cough, dyspnea and atypical chest pain. We describe the case of a 30 year old female with a 3 month history of unexplained cough. Extensive workup and empiric treatment for the standard causes of cough were unsuccessful. More detailed workup including bronchoscopy, endoscopy, pulmonary function testing and otolaryngology evaluation was normal. Computed tomographic (CT) scan and Magnetic resonance imaging (MRI) of the chest revealed a 5.8 cm pericardial cyst in the left cardiophrenic angle. Video assisted thorascopic surgery (VATS) was performed for removal of the cyst and the cough resolved completely postoperatively. |
Pericardial cysts are uncommon intrathoracic lesions, typically located in the cardiophrenic angles. While most pericardial and mediastinal cysts are incidental findings on imaging, some are associated with symptoms including shortness of breath, pleuritic chest pain and nonproductive cough. We report the case of a woman who presented with no complaints other than nonproductive cough which resolved completely after surgical removal of a pericardial cyst.
A 30 year old woman presented in March 2010 to our institution with a 6 week history of nonproductive cough. She had a prior history of atrioventricular (AV) node modification for AV node reentrant tachycardia and autonomic dysfunction refractory to all medications except low dose Amiodarone. The cough was initially treated at an outside urgent care with antibiotics. Upon her presentation in March, empiric treatment of upper airway cough syndrome (UACS), asthma, and reflux disease was initiated along with more aggressive cough suppression. A thorough physical examination, chest x-ray and pulmonary function testing with methacholine challenge were normal. Amiodarone was discontinued early in the course to eliminate it as a possible contributor to her cough, and a non contrast chest computed tomographic (CT) was done which showed no evidence of interstitial lung disease or infiltrate. The patient was admitted to our hospital in March with no relief of the cough and worsening chest wall pain due to two fractured ribs she suffered as a result of her incessant cough. A nuclear medicine perfusion/ventilation scan and transthoracic cardiac echo done during admission were read as normal. The patient was seen by the inpatient pulmonary consult team and a recommendation was made for a trial of oral prednisone for possible post- infectious reactive airway disease. At discharge the patient was instructed to finish the course of prednisone and given oral pain medications and a cough suppressant. An outpatient bronchoscopy showed normal endobronchial anatomy, mild tracheobronchitis, and no endobronchial lesions. Cytology and cultures for acid fast bacilli, fungal and routine organisms from the bronchoscopy were negative. A high resolution chest CT revealed a 2.9×5 cm water attenuation mass in the left cardiophrenic angle consistent with a pericardial cyst. Additional investigation undertaken to elucidate the cause of the cough included a normal esophagogastroduodenoscopy (EGD) with biopsy. Endoscopic ultrasound revealed the known cyst above the left diaphragm with no solid component and no associated mediastinal lymphadenopathy. Laryngoscopic evaluation by the otolaryngology service was unrevealing. The cardiothoracic surgery service was consulted and recommended video-assisted thorascopic surgical resection (VATS) of the pericardial cyst. Prior to surgery, an magnetic resonance imaging (MRI) with and without contrast was performed. T2-weighted images revealed a 5.8×3.1×2.5 cm non-enhancing fluid signal within the left cardiophrenic angle confirming the location and extent of the cyst (Figure 1). An uneventful VATS resection of the pericardial cyst was performed in June 2010. The cyst lay beneath the parietal pleura and tracked a distance of approximately 6 cm from the apex of the pericardium to the antero-inferior most recess of the cardiophrenic angle. Direct pericardial connection was not present. Pathology revealed a transparent, clear, fluid filled pericardial cyst (Figure 2). Postoperatively, the patient had immediate resolution of the cough and had an uneventful recovery.
|
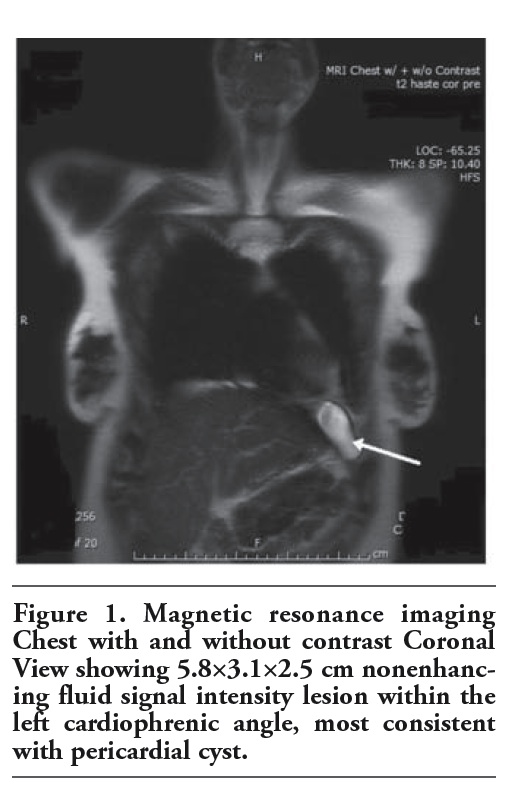
Figure 1. Magnetic resonance imaging Chest with and without contrast Coronal View showing 5.8×3.1×2.5 cm nonenhancing fluid signal intensity lesion within the left cardiophrenic angle, most consistent with pericardial cyst. |
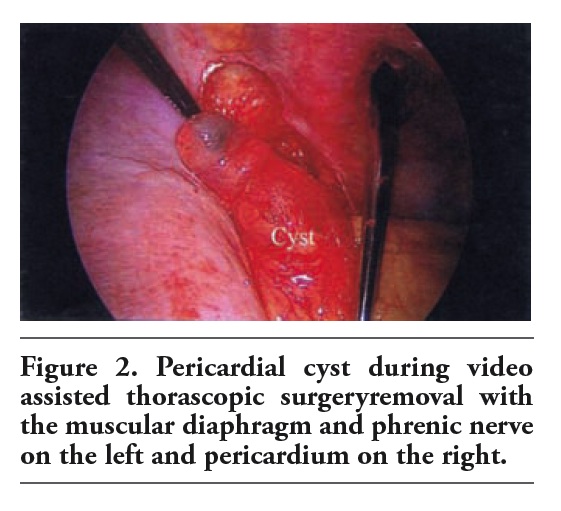 |
Figure 2. Pericardial cyst during video assisted thorascopic surgeryremoval with the muscular diaphragm and phrenic nerve on the left and pericardium on the right. |
We describe the case of a 30 year old woman with a 4 month history of unexplained cough. Systematic empiric treatment for the most common causes of cough [i.e., upper airway cough syndrome (UACS), asthma, and gastroesophageal reflux disease (GERD)] did not eliminate the symptoms. Pulmonary function testing with a bronchoprovocation challenge was normal and bronchoscopy showed no evidence of infection or eosinophilic bronchitis. A high resolution CT scan performed during the workup revealed the presence of a 5 cm pericardial cyst in the left cardiophrenic angle. Endoscopic ultrasound done to further characterize the lesion revealed a simple thin walled cyst with no solid component and no associated lymphadenopathy, making the possibility of malignancy or hydatid cyst unlikely. When there was no other explanation for her persistent unexplained cough, a VATS removal of the cyst resulted in immediate and complete resolution of the cough.
Pericardial cysts are rare mediastinal cysts occurring with an incidence of 1 in 100,000. While they characteristically occur along the right cardiophrenic angle,1 in the case we describe the cyst was located along the left cardiophrenic angle. Patients are usually asymptomatic but may present with a nonproductive cough, shortness of breath, pleuritic chest pain and rarely congestive heart failure.1,2 The reason why a small pericardial cyst should cause symptoms is often elusive. There is clear evidence that vagal afferent nerves regulate involuntary coughing. It is possible the mechanism of the cough is the presence of vagal sensory receptors within the lungs and airways that discharge into the vagus and transmit information to the central nervous system.3 There is much debate about whether asymptomatic mediastinal cysts should be resected as the relationship of cysts to symptoms remains unclear.4,5 In this case the relationship of the cyst to her cough was clearly defined as her 4 month cough resolved immediately after VATS. Additionally, most mesothelial and thymic cysts can be handled by VATS which lowers the risk of morbidity and mortality. Although pericardial cyst is a rare cause of symptoms it should be considered in the differential diagnosis as a cause of unexplained cough.
1. Duwe BV, Sterman DH, Musani AI. Tumors of the mediastinum. Chest 2005;128:2893-909.[PubMed]
2. Gürsoy S, Ozturk A, Ucvet A, Erbaycu AE. Benign primary cystic lesions of mediastinum in adult: the clinical spectrum and surgical treatment. Arch Bronconeumol 2009;45:371-5.[PubMed]
3. Hargreaves M, Channon K. Mechanism of pacemaker induced cough. Br Heart J 1994;71:484-6.[PubMed]
4. Takeda S, Miyoshi S, Minami M, et al. Clinical spectrum of mediastinal cysts. Chest 2003;124:125-32.[PubMed]
5. Irwin, RS, Baumann MH, Bolser DC, et al. Diagnosis and management of cough executive summary: ACCP evidence-based clinical practice guidelines. Chest 2006; 129:1S-23S.[PubMed]
[TOP]