Eiki Ichihara1, Nagio Takigawa1, Katsuya Kato2, Yasushi Tanimoto1, Ichiroh Yamadori3, Katsuyuki Kiura1, Mitsune Tanimoto1
1Department of Respiratory Medicine, Okayama University Hospital, Japan; 2Department of Radiology, Okayama University Hospital, Japan; 3Laboratory Investigation Section, Okayama University Hospital, Japan
Correspondence: Nagio Takigawa, Department of Respiratory Medicine, Okayama University Hospital 2-5-1 Schikata-cho, Okayama 700-8558, Japan. Tel: +81.86.235.7229 - Fax: +81.86.232.8226. E-mail: ntakigaw@md.okayama-u.ac.jp
Key words: pulmonary alveolar proteinosis, gravitation effect, interlobular septal thickening
Conflict of interest: the authors report no conflicts of interest.
Received for publication: 2 March 2011.
Revision received: 24 March 2011
Accepted for publication: 24 March 2011.
©Copyright E. Ichihara et al., 2011
Licensee PAGEPress, Italy
Chest Disease Reports 2011; 1:e2
doi:10.4081/cdr.2011.e2
AbstractAn 80-year-old man presented with heterogeneous ground glass opacity, with interlobular septal thickening in the left lower lobe. The histology of a surgical lung biopsy showed alveolar proteinosis. Computed tomography revealed that the ground glass opacity and interlobular septal thickening observed dorsally in the supine position migrated to the ventral side in the prone position. To the best of our knowledge, this is the first report of a posture-dependent migrating shadow in a patient with pulmonary alveolar proteinosis. |
Pulmonary alveolar proteinosis (PAP) was first reported by Rosen et al. in 1958.1 Its etiology is considered to be altered surfactant homeostasis, causing the accumulation of surfactant in alveolar air spaces.2 Computed tomography (CT) of PAP demonstrates air-space consolidation, ground glass opacity (GGO), and thickened interlobular septa, or what we call having a crazy paving appearance.2 Here, we describe migration of the CT shadow of PAP with posture change.
An asymptomatic 80-year-old man presented with a worsening abnormal shadow on chest radiographs during 7 months. He was a current smoker with a 26 pack year history. He had worked as a technician mixing concrete for 5 years and crushing stones for 4 years. The physical examination was non-specific. A chest radiograph revealed increased reticular and linear shadows in the left lower lung field. CT demonstrated a heterogeneous opacity with interlobular septal thickening in the left lower lung, which was compatible with the crazy paving appearance (Figure 1A). Bronchoscopy was performed for diagnostic purpose. Bronchoalveolar lavage fluid (BALF) obtained from the left anteriorbasal segment was transparent and deep yellow. The total cell count was increased to 11.4×105 /mL, and the differential count consisted of 87.6% lymphocytes. The surfactant protein D level in the BALF was markedly elevated to 14.7 µg/mL, versus around 0.9 µg/mL in healthy individuals.3 Cultures of the BALF did not grow bacteria, fungi, or mycobacteria. No anti-granulocyte-macrophage colony-stimulating factor (anti-GM-CSF) was detected in the BALF or serum. We that suspected this case was PAP, cryptogenic organizing pneumonia, interstitial pneumonia, or lymphangitis carcinomatosa. He had no subsequent treatment after the bronchoalveolar lavage. After one month, the shadow of the left lower lung progressed without any symptoms. He underwent video-assisted thoracoscopic surgery to obtain tissue from the left lower lung. The pulmonary alveolar architecture was unaltered and some granulomas indicated pneumoconiosis. Most of the air space was empty, but some alveoli contained macrophage aggregates and finely granular eosinophilic material that stained weakly with periodic acid Schiff and immunohistochemically with antibody against surfactant protein A (Figure 1B). The patient was diagnosed with PAP related to pneumoconiosis. A chest CT performed 2 weeks postoperatively did not show any significant differences, except a left pleural effusion due to the operation. However, a CT taken in the prone position after lying in the prone position for 2 hours demonstrated that the GGO moved to the ventral part of the lower lobe and the interlobular septal thickening disappeared (Figure 1C, D). The patient was followed closely without therapy, and the CT shadow disappeared completely after 3 years.
|
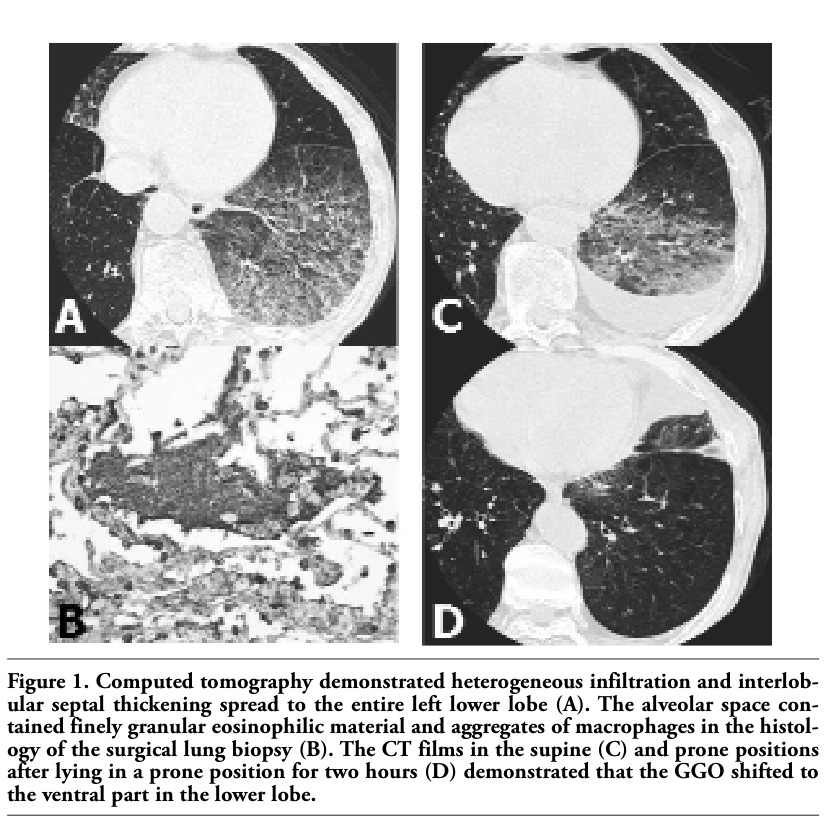
Figure 1. Computed tomography demonstrated heterogeneous infiltration and interlobular septal thickening spread to the entire left lower lobe (A). The alveolar space contained finely granular eosinophilic material and aggregates of macrophages in the histology of the surgical lung biopsy (B). The CT films in the supine (C) and prone positions after lying in a prone position for two hours (D) demonstrated that the GGO shifted to the ventral part in the lower lobe. |
We described a moving shadow due to the effect of gravitation in a patient with PAP. When we found that the histopathological manifestations were much less than we expected from the CT findings and noticed that the horizontal appearance of the upper level of the GGO (Figure 1C) was like an air fluid level, we decided to perform CT in the prone position. The shadow observed dorsally in the supine position on CT migrated to the ventral side in the prone position (Figure 1D). A similar phenomenon could have happened during the operation (i.e., in the right lateral decubitus position), which might explain why the histological findings were relatively modest compared with the radiographic findings, despite obtaining the desired pulmonary tissue. Transparent BALF, which appears milky in typical PAP, might imply a lower protein content causing decreased viscosity of the substance filling the alveoli. The decreased viscosity would enable this substance to migrate readily due to the gravitation effect.
PAP in adult patients is classified into idiopathic PAP associated with anti-GM-CSF antibodies and secondary PAP associated with dust inhalation (e.g., silica, titanium, aluminum) or hematologic malignancies.2,4,5 Typical PAP patients have modest symptoms compared to the radiological findings and about one-third are asymptomatic. When the symptom is moderate to severe, treatments such as supplemental oxygen and whole lung lavage are needed. The efficacy of GM-CSF for idiopathic PAP is reported, but further investigation is needed.2,4,5
PAP induced by pneumoconiosis has been reported6,7 and no anti-GM-CSF antibodies were detected in the blood or BALF in secondary PAP.8 Because the patient was a technician mixing concrete and crushing stones, he aspirated silica or other inorganic dusts. Therefore, this case was considered to be secondary PAP related to pneumoconiosis. Pneumoconiosis is usually a characterized by a diffuse pulmonary fibrosis induced by long term exposure of silica or other inorganic dusts. In this patient, the pulmonary alveolar architecture was unaltered and some granulomas indicated pneumoconiosis pathologically. Huge inhalation of silica is reported to cause the complication of pneumoconiosis and PAP called silicoproteinosis, but different from the current case, silicoproteinosis was reported to be acute onset and a poor prognosis.9,10 We believe that the present case was caused by the inhalation of dusts other than silica.
In conclusion, to the best of our knowledge, this is the first report of a posture-dependent migrating GGO of PAP.
1. Rosen SH, Castleman B, Libow AA. Pulmonary alveolar proteinosis. N Eng J Med 1958;258:1123-42.[CrossRef][PubMed]
2. Ioachimescu OC, Kavuru MS. Pulmonary alveolar proteinosis. Chron Respir Dis 2006;3:149-59.[CrossRef][PubMed]
3. Kuroki Y, Takahashi H, Chiba H, Akino T. Surfactant proteins A and D: disease markers. Biochim Biophys Acta 1998;1408:334-45.[PubMed]
4. Uchida K, Beck DC, Yamamoto T, et al. GM-CSF autoantibodies and neutrophil dysfunction in pulmonary alveolar proteinosis. N Eng J Med 2007;356:567-79.[CrossRef][PubMed]
5. Greenhill SR and Greenhill DN. Pulmonary alveolar proteinosis: a bench-to-bedside story of granulocyte-macrophage colony-stimulating factor dysfunction. Chest 2009;136:571-7.[CrossRef][PubMed]
6. McCunney RJ, Godefroi R. Pulmonary alveolar proteinosis and cement dust: a case report. J Occup Med 1989;31:233-7.[CrossRef][PubMed]
7. Sauni R, Järvenpää R, Iivonen E, et al. Pulmonary alveolar proteinosis induced by silica dust? Occup Med (Lond) 2007;57:221-4.[CrossRef][PubMed]
8. Lin FC, Chang GD, Chern MS, et al. Clinical significance of anti-GM-CSF antibodies in idiopathic pulmonary alveolar proteinosis. Thorax 2006;61:528-34.[CrossRef][PubMed]
9. Xipell JM, Ham KN, Price CG, Thomas DP. Acute silicoproteinosis. Thorax 1977;32: 104-11.[CrossRef][PubMed]
10. Marchiori E, Souza CA, Barbassa TG, et al. Silicoproteinosis: high-resolution CT findings in 13 patients. AJR Am J Roentgenol 2007;189:1402-6.[CrossRef][PubMed]
[TOP]